Are you the payer engineer who inherited "wire up consent" as a one-line ticket on the CMS-0057-F backlog? The truth is, consent, attribution-of-record, and audit trails are the parts of the rule that trip teams late in the project, because they cut across all four APIs instead of living in one of them. If you want a sober tour of how these pieces snap together, keep reading, and if you want the broader vendor landscape after that, you can browse the FHIR review hub for context.
What the Rule Actually Asks You to Prove
CMS-0057-F does not just require the Patient Access, Provider Access, Payer-to-Payer, and Prior Authorization APIs to exist. It requires you to show, per member and per request, who consented to what, which payer was the source of a claim or authorization, and what happened at every access point. The default posture differs by API. Patient Access is opt-in, driven by the member through their own app. Provider Access is opt-out, meaning the member is enrolled by default and can withdraw. Payer-to-Payer at concurrent-coverage start is also opt-in. Getting the defaults wrong is the fastest way to draw an audit finding.
Three FHIR resources carry most of the load here:
- Consent captures the member's decision, its scope, its provisions (data classes, date ranges, actors), and when it was captured or revoked.
- Provenance records who created or transformed a resource, which is how you keep attribution-of-record when a member moves between payers.
- AuditEvent logs every read, write, and export across the four APIs.
Wiring Consent Into Each API
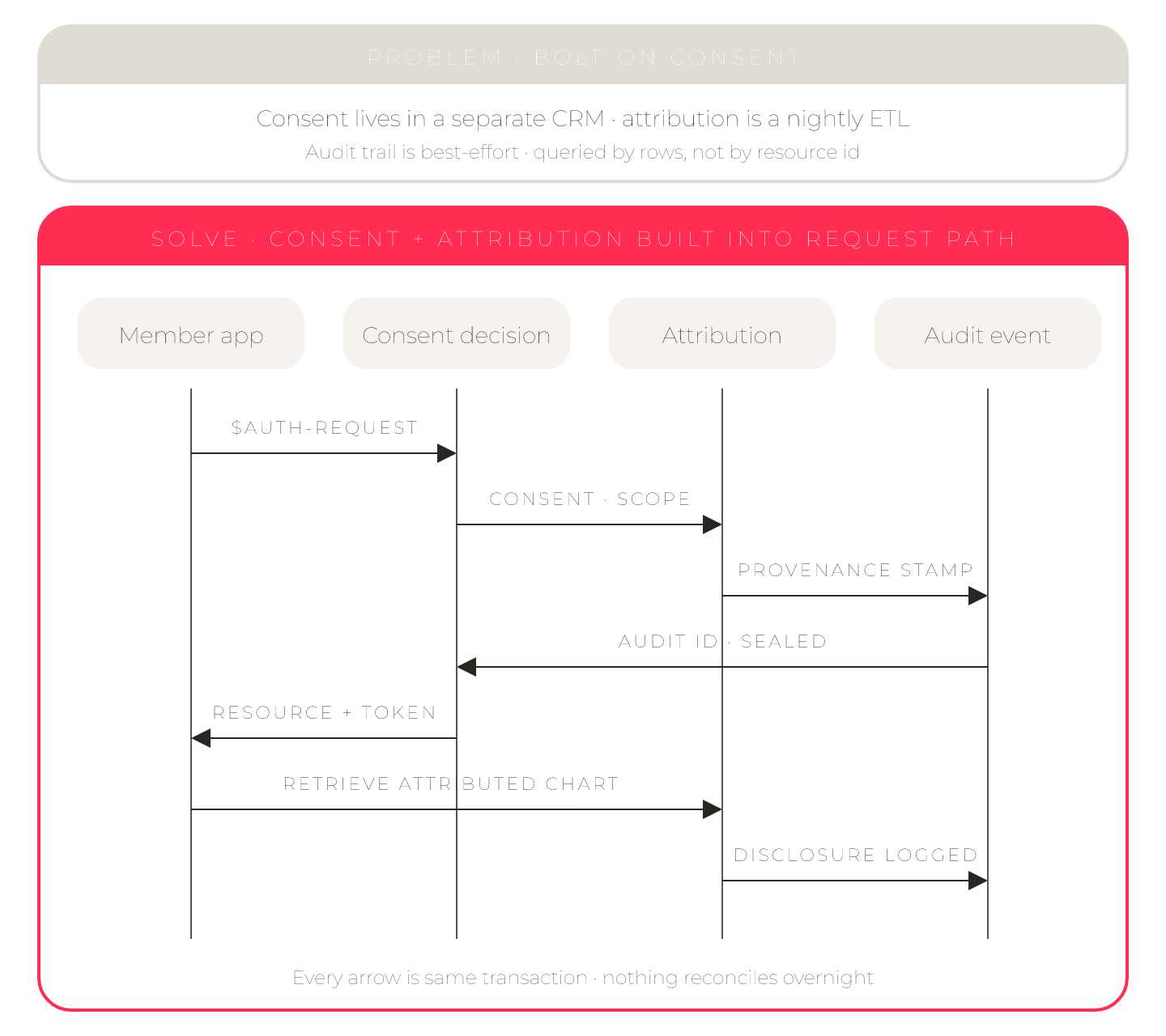
Start at the identity provider. Your IdP is the natural place to prompt for consent during member or provider authentication, then hand a signed assertion back to the FHIR layer. From there, your integration engine writes a Consent resource keyed to the member and to the specific API scope. Keep the decision granular. A Consent.provision for Patient Access should not silently authorize Provider Access data classes. When a member revokes, do not delete the old Consent; write a new one with status inactive and a revocation timestamp, and let your query layer honor the latest active record.
Attribution-of-record is where teams underestimate the work. When a member switches from Payer A to Payer B, the incoming Payer-to-Payer bundle needs Provenance entries that name Payer A as the source of each historical claim, medication, or prior auth. Do not flatten those into your own namespace. If you rewrite Encounter.serviceProvider or drop the origin metadata, you lose the ability to answer "who said this first" during a dispute.
Vendor evaluation typically pits point CMS-0057-F services against reusable FHIR stores like Aidbox with an embedded compliance layer such as Payerbox from Health Samurai, and the consent-plus-audit story is often where the two shapes diverge in practice. Point services tend to ship consent for one API and leave the cross-API stitching to you.
For deeper detail on how the integration surface behaves at the boundary, the sibling piece on FHIR integration tools for payer data exchange is worth a scan, and the prior auth tools that span X12 278 and FHIR PAS covers the request-shaped counterpart.
Retention, Revocation, and the Audit Pipeline
AuditEvent volume is the surprise line item. Every Patient Access read, every Provider Access pull, every Payer-to-Payer transfer, and every Prior Auth submission needs an event. Plan for a write-optimized store, a retention policy that matches your legal hold, and a member-facing view where a subscriber can see who touched their record. Revocation should propagate within minutes, not overnight batches. If your pipeline meets those three bars, the compliance officer conversation gets a lot shorter.
Sources
- spec, HL7 Da Vinci PDex v2.2.0, evergreen — PDex Provider Access Consent Profile (opt-out semantics for Provider Access API)
- PDF, CMS, 2024 — CMS-0057-F Interoperability and Prior Authorization Final Rule (canonical text; attribution + opt-out requirements)
- spec, HL7, evergreen — FHIR R5 AuditEvent resource (audit trail model for read/write/export across the four APIs)